
Relationships
 THE WHOLE BIPOLAR SEX THING
THE WHOLE BIPOLAR SEX THING

Why bipolars may make the best lovers - or worst.
by John McManamy
Why bipolars may make the best lovers - or worst.
by John McManamy
A LOT has been written on sex and a lot on bipolar but virtually nothing on the two together. Let's change that ...
Choosing a Partner
Back in 2002, Rutgers anthropologist Helen Fisher. scanned the brains of young people in love. When the subjects looked at photos of their sweethearts, the right ventral tegmental area (VTA) - the dopamine-sensitive region in the midbrain that mediates pleasure and reward - lit up like a Christmas tree. At the same time, the amygdala - fear central - went silent.
In evolutionary terms our genetic future is too important to entrust to the thinking parts of the brain.
One thing the brain science is emphasizing loud and clear is that our reason guides us far less than we think. This is not necessarily a bad thing. What we are learning is that the cortical (thinking) areas of our brain need input from the limbic (emotional) areas of the brain in order to figure things out. When the chips are down, we choose what "feels good" to us and are repelled by what "feels bad."
This applies whether we are buying a car or voting for a political candidate or choosing a partner, with the VTA essentially calling the shots and the cortical areas rationalizing the choice. Again, this is not necessarily bad. The cortex can be flooded with too much information and easily hoodwinked into making bad decisions.
How Bipolar Enters Into All This
Where you find love you will find dopamine. Dopamine is vital to mental alertness, cognition, motivation, not to mention feelings of pleasure, high energy, anticipation, and gratification. In short, on dopamine we feel alive. But crank up the dopamine and we get anxious, paranoid, manic, over-energetic, and addictive. We make bad - often catastrophic - decisions. Tamp down the levels and we are depressed, lethargic, and indifferent. Again, we make terrible decisions, or we fail to make decisions.
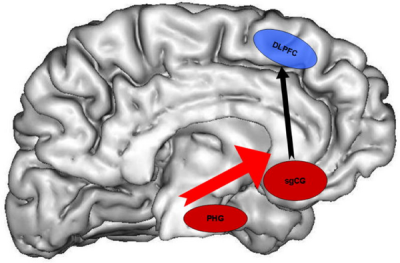
Bipolar is a very complex illness, but no matter what the actual cause and effect, we know we are certain to find an over-active or under-active dopamine circuit somewhere. Below is a rendering of the brain that shows increased signaling between two different regions displayed by episode-free individuals with bipolar I in response to images of facial expressions. The control subjects also displayed increased signaling, but to a far lesser extent.




SIGN UP FOR MY FREE EMAIL NEWSLETTER
Perhaps we engage in sex with greater intensity than others. Perhaps not. But what seems plausible is that we experience greater subjective feelings of intensity. Whatever is going on, our brains are reacting like photo-sensitive paper to light. This intensity carries over to feelings of attachment. At once, we are euphoric and obsessed and anxious - the kind of feelings "normal" people have when they are in love. But can we truly trust our own feelings? Are we really in love, or is it our brains simply running away on us?
Are we about to make a catastrophic decision - again?
Challenging the Conventional Wisdom
The conventional wisdom is that (hypo)mania increases our sexual drive - often to the point of excess - while depression has the opposite effect. Indeed, this is borne out by our personal experiences. This from "Ellen":
There are times I'm driving and I get so wound up I'll call my husband and tell him to meet me 'cause I need to have sex.
Goodwin and Jamison in their 2007 "Manic-Depressive Illness" note that Aretaeus of Cappadocia in the second century AD observed "a period of lewdness and shamelessness exists in the highest type of [manic] delirium."
The authors cite a number of studies showing increased sexual interest and behavior during mania or hypomania, and the DSM makes it official by including "sexual indiscretions" in manic and hypomanic episodes. It also notes "decrease in sexual interests or drive" during depression.
Okay, time to challenge that notion. A 2006 NIH-funded study of a large teen population found that those who were depressed were far more likely to engage in risky behaviors such as drug use and sex. The study corroborates earlier findings.
One aspect of depression is a feeling of being "clinically dead but breathing," the very opposite of the "feeling alive" states of mind we experience in pure mania and hypomania. But something else also tends to be going on - intense psychic pain. If the clinically dead aspect of depression is about feeling too little, our psychic pain is about feeling too much. In this tortured state of mind we tend to be desperate for release, and seek it in a variety of ways - from attempting suicide to over-eating and over-sleeping to alcohol and drug abuse to "retail therapy" to the flood of feel-good hormones from a warm embrace.
The feeling may quickly wear off, but so what? People who have never experienced depression cannot possibly understand.
Thus both sides of the bipolar equation find us at risk, up as well as down. Yes, it is true that we are more likely to lose interest in sex when we are depressed, but this should not mask the fact that in certain instances the very opposite may occur, replete with the full menu of life-altering consequences. Psychic pain has that kind of effect on us.
Do Bipolars Make the Best Lovers?
Does hypersexuality in mania and hypomania actually translate to being better in bed? We have no evidence.
What is reasonable to assume is that our ups intensify all our experiences, whether listening to music, enjoying food, watching a sunset, or having sex. Even our downs can add layers of richness to our existence.


But is it possible for those close to us to experience our subjective realities? The answer appears appears to be yes. Our states of mind can be contagious. Wrote Kay Jamison of Virginia Woof, citing one of her social circle: "I always felt on leaving her that I had drunk two excellent glasses of champagne. She was a life-enhancer."
But the very intensity of our world can also be very frightening to others. Virginia Woolf may have lit up her Bloomsbury circle, but she also drove poor husband Leonard nuts. Likewise, the intensity factor has a way of drowning out the rest of our surroundings, including the people around us. When "Me" is involved at the expense of "We," bad things tend to happen.
So - let's make a few wild guesses about what happens when we take our enhanced subjective realities to the bedroom. When things go right, it appears that the intensity we bring to the moment jumpstarts the "normal" partner's intensity, and next thing both partners are experiencing the type of cosmic union you read about in the poetry of Rumi.
Sample verse: "You are the sky my spirit circles in."
But maybe things get too intense for the comfort of our partner, perhaps to the point where he or she no longer feels safe. Maybe we are so into our own needs and desires that we lose sensitivity to those of our partner. We fail to pick up vital signals. We fail to make the necessary adjustments. Sex is mind-blowing enough without adding bipolar to it. Thus, if we are prepared to brag about how bipolars make the best lovers, we also need to accept the fact that there are times when we are probably the worst.
The "Bipolar-By-Proxy" Complication
Jumpstarting our partners may have the effect of turning them into "bipolar-by-proxy." This is wildly speculative, but let's run with it. If our partner is feeling the same kind of intensity we are feeling, with similar dopamine surges, then their capacity to make rational decisions may be as impaired as ours, perhaps more so. We at least have an experiential context to place our current state of intensity. Our partner may confuse this novel experience with love.
The Meds Factor
Those on medications frequently complain about their lost sex drive. But other patients express relief over finding their over-active sex drives moderated to the point of being able to engage in normal loving relationships for a change, without fear of going off the rails.
Clearly our sexual drive is a vital part of who we are and how we relate to those around us. In no way should what amounts to long-term chemical castration be regarded as an acceptable trade-off for our own emotional stability.
The reality, though, is that treatment and eventual recovery involve a number of short and medium-term trade-offs. Unfortunately, our psychiatrists are very bad at explaining this to us, much less working with us on a six-to-twelve month strategy aimed at lowering our doses to less debilitating levels. Too often, we are left wondering:
Is this what it is going to be like for me - for the rest of my life?
My guess is that oncologists are much better at going over the long-term game plan with their patients. This would explain why the meds compliance rates for cancer patients are so much higher.
What would the promise (no guarantees) of light at the end of the tunnel be worth to you? Six months with no sex drive? A year? You are not being unreasonable insisting on a long-term plan involving a life of full-function.
Reviewed July 13, 2016
NEW!
Follow me on the road. Check out my New Heart, New Start blog.






